Research Article
Volume 1 Issue 3 - 2016
Patient Education on Care of Diabetes for Patients with Diabetic Foot Problems
Lim Qiao Yan Eda1, Chan Shu-Yi Claire2, Malhotra Rishi3, Wee Lin4, Ang Yi Yen Zest5, Wong Le Yi Joy6, Lim Kai Bing, Danson7 and Aziz Nather8*
1,2,3,4,5,6,7,8Department of Orthopaedic Surgery, National University Health System, Singapore
*Corresponding Author: Associate Professor Aziz Nather, Senior Consultant University Orthopaedics, Hand & Reconstructive Microsurgery Cluster National University Health System, Singapore.
Received: December 15, 2016; Published: December 21, 2016
Abstract
The key to the management of diabetic foot complications is prevention. To achieve this, good education guides must be made available to teach patients on care of diabetes, foot care and foot wear. Whilst several guides are available in literature, many are written in technical language, making it difficult to comprehend by patients.
The objectives of this project were firstly to design a survey questionnaire covering as comprehensively as possible all aspects patients need to know on the care of diabetes and secondly, to design a new education package based on the results better suited to teach patients on all important aspects of diabetes care.
The survey was conducted on a cohort of 40 people with diabetic foot problems managed by the National University Hospital Diabetic Foot team headed by the senior author (A. Nather) from February 2014 to May 2014. The package was then specifically designed to cover all gaps in knowledge on diabetes care. It is written in English in an easy-to-read fashion and produced with good illustrations to make them easier to understand.
The percentage of correctly answered questions for the individual questions from each section ranges from 53 to 85% (General knowledge), 98% (Diagnosis), 80 to 85% (Medication), 25 to 98% (Treatment) and 10 to 93% (Healthy lifestyle).
Our survey showed that whilst current education booklets exist, they do not cover gaps in knowledge of diabetes care that patients need. This newly designed booklet addresses these gaps to help educate patients more effectively.
Keywords: Foot Care; Foot Wear; Diabetes Care; Diabetic Foot Problems; Education booklets
Abbreviations: NIL
Introduction
Diabetes mellitus is one of the top four chronic diseases that plague one million Singaporeans [1]. Since the early 90s, diabetes has been deemed as a priority condition for disease control in Singapore. The increasingly sedentary lifestyles and aging population in Singapore has led to a rising proportion of individuals diagnosed with diabetes [2]. If not properly managed, diabetes can lead to the onset of severe complications which may endanger patients’ lives. According to the Ministry of Health, Singapore, the high medical costs of treatment usually arise due to the onset of complications when treatment is delayed. Treatment is often delayed as patients lack knowledge on the early identification and proper management of diabetes. The effective management of diabetes requires control over an interplay of factors that affect blood glucose level in diabetic patients [3]. These include dietary habits, daily lifestyle and method of coping with diabetes. As most of the factors are closely related to patient behaviour, it appears evident that the attainment of long-term management is the consequence of effective patient education. Hence, patient education is crucial for early prevention [2].
Education has been proven to contribute significantly to sustained success of diabetes management through the prevention or delay of long-term complications [3,4]. A study conducted by Tan., et al. in a government outpatient clinic showed that educating patients on general diabetes knowledge led to an improvement in their knowledge of diabetes, self-management and long-term regulation [5]. Another study by Tham., et al. in 2004 found that even though the state of diabetic education has improved tremendously, ‘some key aspects of diabetes and self-care were either missed out, or the subjects forgot or did not understand their importance, resulting in their ignorance’ [6].
The objectives of this research were to determine the level of knowledge patients have about diabetes in Singapore and subsequently, produce a directed education package that addresses these gaps in knowledge that patients have.
Materials and Methods
This pilot study was split into four phases: designing of survey questionnaire, carrying out the survey, designing a comprehensive syllabus for producing a new education package to address all the gaps in knowledge that patients may have (Figure 1).
Figure 1: Phases in this pilot study.
Designing the Survey Questionnaire
Literature review was carried out on previous research papers which focused on developing effective indicators to determine how much patients know about diabetes [7-10]. Elements that increased the accuracy of survey questionnaires in determining the level of knowledge patients have, such as the ‘I don’t know’ option and the multiple-choice format, were retained while the lack of scope in previous questionnaires was improved on.
The re-developed survey questionnaire was produced in the multiple-choice format. All questions featured an ‘I Don’t Know’ option to reduce the ambiguity of whether patients know the answer to a certain question. Simple and concise terms were used for easy communication with patients. The survey questionnaire was also structured to cover all topics in the syllabus for the education package. Questions were spread evenly over the four main areas. These areas include ‘What is Diabetes?’ (9 questions), ‘Diagnosis’ (1 question), ‘Treatment’ (7 questions) and ‘Healthy Lifestyle’ (8 questions) (Table 1). This ensured that the survey questionnaire was able to give a holistic review of what patients know about diabetes.
What is Diabetes?
- DM results in our blood glucose level becoming:
a. Low b. High c. I don’t know
- DM is more likely to develop in obese people.
a. Yes b. No c. I don’t know
- The normal range for blood glucose level is:
a. 1-3 mmol/l b. 4-8 mmol/l c. 9-15 mmol/l d. I don’t know
- The common symptoms of DM include:
a. Increased urination b. Increased hunger & thirst
c. Weight Loss d. All e. I don’t know
- If poorly controlled, DM will develop complications such as
a. Kidney Failure b. Blindness c. Weight Loss d. All
e. I don’t know
- A patient with DM is more prone to infections and will not recover quickly.
a. Yes b. No c. I don’t know
- High blood sugar will result in breathlessness, fatigue and nausea.
a. Yes b. No c. I don’t know
- Low blood sugar can make a person confused or aggressive.
a. Yes b. No c. I don’t know
- If a patient is having flu, he/she should:
a. Take less insulin or oral anti-diabetic medicine
b. Drink less liquids c. Take your own flu medication
d. Test your blood glucose level before deciding
e. I don’t know
Diagnosis
- DM is diagnosed by blood glucose tests
a. Yes b. No c. I don’t know
Treatment
- All DM patients can be controlled with medication alone.
a. Yes b. No c. I don’t know
- DM patients should carry glucose tablets or sweets on them when going out
a. Yes b. No c. I don’t know
- Patients should maintain a healthy weight and check their BMI regularly.
a. Yes b. No c. I don’t know |
- What should a patient do if he/she experiences dizziness or fainting spells?
a. Eat or drink something sweet b. Inject insulin
c. Drink water d. Rest and wait for it to pass
e. I don’t know
- What is the acceptable HbA1c blood glucose level?
a. 4-6.4% b. 6.5%-8% c. 8-12% d. I don’t know
- How often should patients visit the doctor for eye check-ups?
a. Monthly b. Once every 6 months c. Once a year
d. I don’t know
- How often should patients visit the doctor for feet examinations?
a. Monthly b. Once every 6 months c. Once a year
d. I don’t know
Healthy Lifestyle
- DM patients can use artificial sweeteners which have no effect on blood sugar level.
a. Yes b. No c. I don’t know
- Patients should limit their intake of carbohydrate as it affects the blood glucose level most significantly.
a. Yes b. No c. I don’t know
- What is the ideal daily calorie intake for diabetic patients?
a. 1000 calories b. 1800 calories c. 2600 calories
d. I don’t know
- What effect does unsweetened fruit juice have on blood glucose level?
a. Lowers it b. Raises it c. No effect d. I don’t know
- How often should a diabetic patient exercise weekly?
a. Everyday b. Twice Weekly c. 5 times weekly
d. I don’t know
- It is important to check your blood glucose level before and after exercising.
a. Yes b. No c. I don’t know
- Smoking increases the risk of amputation in diabetic patients.
a. Yes b. No c. I don’t know
- Alcohol results in an increase in blood sugar level.
a. Yes b. No c. I don’t know
|
Table 1: Survey questions are spread evenly over four core topics.
Clinical Setting and Method of Conducting the Survey
This study was a randomized pilot study conducted in the National University Hospital, Singapore. The survey questionnaire was conducted over a period of 70 days from 26 February 2014 to 6 May 2014. Subjects were chosen from diabetic patients with foot problems managed by the National University Hospital Diabetic Foot Team headed by the senior author (A. Nather). 1 patient had Type 1 diabetes and 39 patients had Type 2 diabetes. They were aged 29 to 72 years old. They were able to speak English, Mandarin, Malay or Hokkien. Those who were too ill to be interviewed were excluded. Informed consent was obtained and participation was voluntary. A system of positive point allocation was employed with one points awarded for a correct answer but none for incorrect or unsure answers. The maximum possible score was 25.
Designing the Education Package
Apart from taking into consideration results from the survey questionnaire, the National University Hospital Diabetic Foot Team also conducted a thorough review of available print education resources in Singapore which include both booklet (Figure 2) and online website (Figure 3).
Figure 2: Booklet by Health Promotion Board.
Figure 3: Website managed by Diabetic Society of Singapore.
At present, the National University Hospital uses the ‘BE aWARE of Diabetes’ booklet produced by the Health Promotion Board, Singapore (Figure 2). This booklet covered a reasonable scope of information. However, some information presented was too wordy and unnecessary which may not be so effectively conducted by patients. Texts which are difficult to comprehend and take too long to read will not be able to hold the attention of patients. The essence of key points will be lost.
Certain practical information that patients need to know are also unavailable. For instance, important information on what patients should do and take note of before, during and after exercising was not included in any of the current education sources in Singapore.
Following the review of current resources and the incorporation of results from the survey questionnaire, the team designed a new syllabus that not only emphasized on areas patients were lacking in but covered a holistic scope of diabetes knowledge.
The booklet produced had key features specially designed so that information was presented in a more effective manner. Sentences were kept short and concise. Only knowledge important for patients was included. More tips and guidelines were given in the booklet as it would be more convenient for patients with a fixed and direct set of instructions to follow (Figure 4).
Figure 4: Tips and guidelines available in the booklet.
Formatting of the booklet was also simple but with more colours for easy reading. Illustrations were carefully chosen and designed for patients to better understand (Figure 5).
Figure 5: Simple format with more colours.
Results
A total of 40 subjects were interviewed. All were diabetic patients with foot problems. The average age of this pilot study population was 25 years old. Majority of the respondents received secondary education.
Respondents were the most informed about the method of diagnosis for diabetes with 97.5% (Figure 6) giving correct answers for Q10. On the contrary, this study population was least informed on how often they should visit relevant medical professionals such as podiatrists and specialists for regular check-ups with a minority of 32.5% on average giving correct answers (Figure 6). Patients were also poorly equipped with knowledge regarding the importance of exercise as part of their diabetes management plan. An average of 40% (Figure 6) correct answers were given for the two questions that cover the frequency patients should exercise and things to take note of before and after exercising (Q22 and Q23). More than half of the study population was able to give correct answers on questions that cover the causes of diabetes, the symptoms of diabetes, complications of diabetes, medication, regular monitoring, diet as well as smoking and alcohol consumption with 71.1%, 62.5%, 71.0%, 82.5%, 83.8%, 61.9% and 70.0% on average getting these types of questions correct respectively.
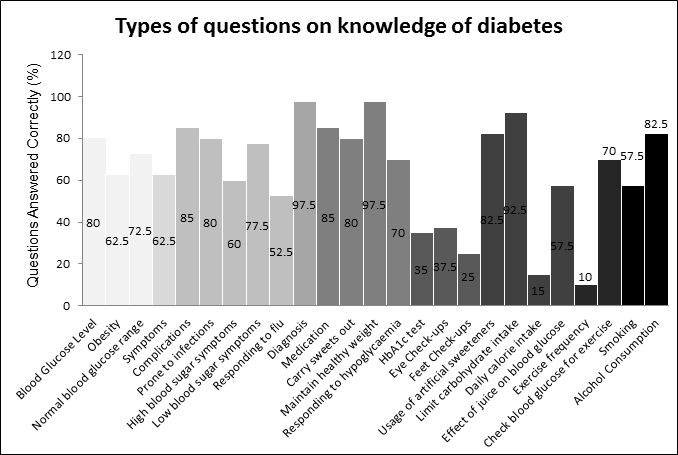
Figure 6: Graph showing the percentage of correct answers given for different categories of questions regarding diabetes.
Causes
Three questions (Q1, Q2 and Q3) covered the causes of diabetes. Of the three questions, respondents were most poorly informed on the negative impact that obesity has on potential patients (Q2). Only 62.5% knew that obesity increases an individual’s chance of suffering from DM. 72.5% of respondents knew the normal range for blood glucose level (Q3). Most respondents were aware that diabetes results due to a higher than normal blood glucose level with 80.0% choosing the correct answer.
Symptoms
Only one question asked about the symptoms of diabetes which include increase urination, weight loss, increased thirst and increase hunger. 62.5% chose the correct option. Interviewers reflected the tendency of respondents to only choose the symptoms that they had personally experienced.
Complications
There were five questions on the complications of diabetes. Generally, 85% and 80% of respondents could list all possible long-term complications of uncontrolled diabetes in Q5 and Q6 respectively. However, they were less informed of the symptoms of short-term complications such as high and low blood glucose level with 60% and 77.5% giving correct answers respectively. Interviewers reflected that respondents listed only the symptoms that they had experienced. Only 25.5% of respondents knew the correct action to take if they were to catch a flu (Q9).
Medication
Two questions which covered medication for the treatment of diabetes revealed that 85.0% of the study population understood that both medication and diet control are required actions to control diabetes. A lower 80.0% knew that it is important to carry sweets on them when going out should they experience a hypoglycemic episode.
Monitoring
97.5% of respondents (Q13) knew the importance of checking their weight and body mass index regularly to ensure that they maintain a healthy weight. A significantly lower proportion of 70.0% (Q14) were aware of what to do in the face of a hypoglycemic episode.
Regular Check-ups
Respondents were the least informed on regular check-ups that they should undergo (Figure 6). Q15, Q16 and Q17 covered the acceptable range for HbA1c test, frequency of eye and feet examinations respectively. For Q16 and Q17, respondents were asked to give answers assuming that they did not have any eye or feet complications due to diabetes yet. However, only 25.5% and 25.0% were able to give the correct answers regarding the frequency of eye and feet examinations.
Diet
Four questions covered the aspect of diet in diabetes management. Respondents were generally aware about what they can consume (Q18), the food type they should limit most stringently (Q19) and the effect of consuming food (Q21). However, only 15.0% knew the ideal daily calorie intake (Q20).
Exercise
The two questions on exercise covered the minimum number of times patients should exercise a week (Q22) and what patients should do before and after exercising (Q23). 70% were aware that they should check their blood glucose levels before and after exercising (Q23). A significantly lower proportion of 10% knew the minimum number of times they should exercise weekly.
Smoking and Alcohol Consumption
82.5% knew that alcohol results in an increase in blood glucose level (Q25). Only 57.5% knows that smoking increases the probability of amputation for a diabetic patient.
Discussion
Generally, results showed that respondents had an acceptable level of knowledge on diabetes but there were areas of deficiency that could be addressed. Even though 80.0% of the respondents knew the cause of diabetes to be high blood glucose level, 28.9% were still unaware of the cause behind their disease. If this percentage is applied to a larger cohort of patients, the number of patients who do not know the cause of diabetes will be extremely significant. For management of diabetes, a major part of the treatment is carried out by the patients in collaboration with their doctors [3]. However, many patients do not stick closely to their treatment plans. In the book ‘Adherence to Long-term Therapies: Evidence for Action’ published by World Health Organisation, it is said that ‘Poor adherence to treatment of chronic diseases (including diabetes) is a worldwide problem of striking magnitude’ [11]. This lack of knowledge about the cause of diabetes is a possible cause of such poor adherence to treatment plans.
Knowing the cause will allow patients to understand the underlying root of their disease and the purpose of the treatments administered for them. This understanding can possibly ensure that patients stick more closely to their treatment course when they know how each treatment plan can help them control their condition. Research conducted by Tham et al revealed that being more informed on the causes and basis of treatment will change practices among half of the patients [7].
When designing the new education package, emphasis was placed on presentation of information in a simple and concise manner. More illustrations were used to make patients understand better. Key words and ideas were bolded (Figure 7). Information was arranged to ensure a smooth flow for better understanding.
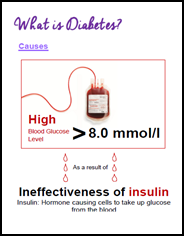
Figure 7: Section on ‘Causes of diabetes’ in Knowing Diabetes.
The survey questionnaire also revealed that only 25.5% and 25.0% know how often to visit a doctor for eye and feet examinations for the prevention of any complications. Regular check-ups are important for the identification of symptoms which will reduce the likelihood of the loss of vision and the need for amputation [12-14]. Yet, information on regular check-ups patients should attend for the early identification of the onset of complications was absent in existing education packages. As such, a section in the new booklet was dedicated to emphasizing the importance of regular check-ups in identifying symptoms of complications. Essential check-ups and their recommended frequencies were listed in a checklist for the convenience of patients (Figure 8). The purpose of each check-up was listed briefly to make sure patients appreciate the importance of each check-up.

Figure 8: Section on ‘Regular Check-ups’ in Knowing Diabetes.
Exercise was another area that patients seemed to be lacking sufficient knowledge in. Only 40% answered questions on exercise correctly. More specifically, respondents scored badly on the question on the minimum number of times patients should exercise weekly where only 10% gave correct answers. During the interview, respondents also reflected that they were unsure of what kinds of exercise are suitable for them, especially for those who have had amputations. As such, to cater more specifically to the needs of diabetic feet patients, the new booklet includes not only the minimum number of times patients should exercise weekly but also gives specific examples of exercises that patients can partake in. For example, different stretches that patients can carry out which are not too strenuous but still fulfill the purpose of exercise. The exercise routine was also included in this new booklet (Figure 9).
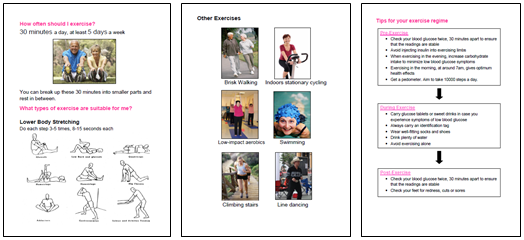
Figure 9: Section on ‘Exercise’ in Knowing Diabetes.
As exercising may result in hypoglycemic episodes, it is important that patients can carry out their exercises safely. A concise flowchart on precautionary measures that patients should take before, during and after exercise was also given to guide patients along (Figure 9). Such practical knowledge were present in existing booklets.
The new booklet also featured a section on advice against smoking and alcohol consumption. From the survey questionnaire, only 67.5% knew of the detrimental impacts of these activities. Little has been written to explain that smoking impacts diabetics even more significantly. There is a lack of information in existing education resources on smoking as well as alcohol consumption. Recommendations for alcohol consumption limit were also given so that patients can keep check of how much they consume should they need to do so.
Conclusion
Our survey showed that whilst current education booklets exist, they do not cover gaps in knowledge of diabetes care that patients need. This newly designed booklet addresses these gaps to help educate patients more effectively.
Acknowledgements: NIL
Conflict of interest: NIL
References
- Ministry of Health, Singapore. Retrieved March 5, 2014.
- Lee WRW. “The changing demography of diabetes mellitus in Singapore”. Diabetes Research and Clinical Practice 50.2 (2000): S35-S39.
- Assal JP., et al. “Patient education as the basis for diabetes care in clinical practice and research”. Diabetologia 28.8 (1985): 602-613.
- Assal JP., et al. “The added value of therapy in diabetes: the education of patients for self-management of their disease”. Metabolism 46.12.1 (1997): 61-64.
- Tan ASL., et al. “Patient education in the management of diabetes mellitus”. Singapore Medical Journal 38.4 (1997): 156-60.
- Tham KY., et al. “How much do diabetic patients know about diabetes mellitus and its complications?” Annals of the Academy of Medicine, Singapore 33.4 (2004): 503-509.
- Dunn S.M., et al. “Development of the diabetes knowledge (DKN) scales: forms DKNA, DKNB, and DKNC”. Diabetes care 7.1 (1984): 36-41.
- Fitzgerald JT., et al. “The reliability and validity of a brief diabetes knowledge test”. Diabetes care 21.5 (1998): 706-710.
- Rothman RL., et al. “The Spoken Knowledge in Low Literacy in Diabetes Scale a Diabetes Knowledge Scale for Vulnerable Patients”. The Diabetes Educator 31.2 (2005): 215-224.
- Quandt SA., et al. “Assessment of a Short Diabetes Knowledge Instrument for Older and Minority Adults”. The Diabetes Educator 40.1 (2014): 68-76.
- Sabate E. “Adherence to Long-term Therapies: Evidence for Action”. Geneva, Switzerland: World Health Organisation (2003).
- “Clinical Practice Recommendation.” American Diabetes Association. Diabetes Care 23 Suppl 1 (2000): S1-116.
- Ryder B. “Screening for diabetic retinopathy”. BMJ 311.6999 (1995): 207-208.
- World Health Organisation. “Prevention of diabetes mellitus: report of a WHO study group”. Geneva: WHO 844 (1994): 1-100.
Citation:
Aziz Nather., et al. “Patient Education on Care of Diabetes for Patients with Diabetic Foot Problems”. Orthopaedic Surgery and Traumatology 1.3 (2016): 85-93.
Copyright: © 2016 Aziz Nather., et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
































;)
;)
;)
;)
;)
;)
;)
;)
;)
 Scientia Ricerca is licensed and content of this site is available under a Creative Commons Attribution 4.0 International License.
Scientia Ricerca is licensed and content of this site is available under a Creative Commons Attribution 4.0 International License.